
Diabetes can affect multiple part of the eye. Spikes in blood glucose can cause fluctuations in vision due to swelling of the lens inside the eye. As the lens swells, its curvature changes and can result in blurred vision. Luckily blurred vision due to lens swelling will usually subside over a few months once the blood sugar levels are brought under control. It is a more serious thing with diabetes starts to affect the retina (the back of the eye).
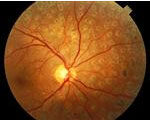
Diabetic retinopathy is a condition which causes progressive injury to the small blood vessels that nourish the retina. Because diabetic retinopathy affects the neurological tissue of the eye, it is a potentially sight-threatening.
There are generally two types of diabetic retinopathy: nonproliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR).
 In NPDR, the damaged retinal blood vessels develop tiny leaks that allow blood and fluid to seep into the surrounding retinal tissue or to form fatty deposits in the retina called exudates. These changes can cause the retina to swell. When swelling or exudates form within the central part of the retina, vision is often reduced or blurred. This is called macular edema because it affects the central part of the retina which is called the macula. Areas of retinal or macular oxygen deprivation can also occur. Blood and other nutrients can no longer be supplied to the retina from damaged small blood vessels.
In NPDR, the damaged retinal blood vessels develop tiny leaks that allow blood and fluid to seep into the surrounding retinal tissue or to form fatty deposits in the retina called exudates. These changes can cause the retina to swell. When swelling or exudates form within the central part of the retina, vision is often reduced or blurred. This is called macular edema because it affects the central part of the retina which is called the macula. Areas of retinal or macular oxygen deprivation can also occur. Blood and other nutrients can no longer be supplied to the retina from damaged small blood vessels.
 PDR differs from NPDR in that it is diagnosed when new abnormal blood vessels begin to form on the surface of the retina, macula or optic nerve. This new blood vessel growth is called neovascularization and usually occurs in response to widespread retinal oxygen deprivation that occurs as part of the NPDR process. The new blood vessels form to help bring a new blood supply to the retina, but these new blood vessels are dangerous. These vessels are fragile and are prone to bleeding. This may cause a vitreous hemorrhage to form. Vitreous hemorrhages can obscure vision for days, weeks or months. New retinal blood vessels often promote the formation of scar tissue within the vitreous and retina which can cause the retina to tear or to detach. A traction retinal detachment can cause significant vision loss depending on how much area of the retina is affected. Neovascularization can also form on the iris and block the flow of fluid inside the eye thereby causing the eye pressure to increase. High eye pressure can result to damage to the optic nerve and may lead to permanent vision loss.
PDR differs from NPDR in that it is diagnosed when new abnormal blood vessels begin to form on the surface of the retina, macula or optic nerve. This new blood vessel growth is called neovascularization and usually occurs in response to widespread retinal oxygen deprivation that occurs as part of the NPDR process. The new blood vessels form to help bring a new blood supply to the retina, but these new blood vessels are dangerous. These vessels are fragile and are prone to bleeding. This may cause a vitreous hemorrhage to form. Vitreous hemorrhages can obscure vision for days, weeks or months. New retinal blood vessels often promote the formation of scar tissue within the vitreous and retina which can cause the retina to tear or to detach. A traction retinal detachment can cause significant vision loss depending on how much area of the retina is affected. Neovascularization can also form on the iris and block the flow of fluid inside the eye thereby causing the eye pressure to increase. High eye pressure can result to damage to the optic nerve and may lead to permanent vision loss.
 DIAGNOSIS
DIAGNOSIS
Both NPDR and PDR can be detected during an examination of the eyes that includes dilation. People who have diabetes should have a dilated eye examination annually. If diabetic retinopathy is diagnosed during the evaluation, other testing may be ordered to determine if treatment is indicated. One test is called Ocular Coherence Tomography (OCT). The OCT takes a scan similar to a photograph of the retina and macula to help localize and quantify areas of macular swelling. Another test is called fluorescein angiography (FA). FA involves injecting dye into the arm of the patient, allowing that dye to travel to the blood vessels of the retina and taking photographs of the dye as it highlights the areas of leakage within the retina. The FA photographs help detect changes that may not be visible on other examinations or on the OCT.
TREATMENT
The results from both the OCT and FA are useful in determining both if and what kind of treatment is indicated for the diabetic retinopathy detected. In some instances, injections of medications into the eye may be indicated to reduce retinal swelling or to reduce neovascularization. Multiple injections may be required over time to manage the retinopathy.
Laser can be used to treat both NPDR and PDR. In NPDR, macular edema may be treated with few focal spots to stop leaks in effort to prevent further vision loss. In PDR, laser is used extensively throughout the peripheral retina to stop the formation of new blood vessel growth. Multiple laser treatments may be required over time to manage the retinopathy.
PREVENTION
If you have been diagnosed with diabetes, you can help lower your risk of developing diabetic retinopathy and other complications of diabetes by controlling your blood sugar. It is important that you take your prescribed medications, maintain a good diet, exercise regularly, keep your blood pressure under control, and avoid smoking as it contributes to blood vessel obstruction. In the early stages of diabetic retinopathy, there are usually no visual symptoms. It is important that all diabetic patients have a comprehensive dilated eye examination once a year.